Somatic Recovery and Multi-Axis Kinetic Entrapment Following a Complex Deconditioning Cascade (2018–2025)
1. Clinical Subject Profile and Longitudinal Baseline.
The subject is a 67-year-old male with a significant 50-year longitudinal history of high-consequence mountain travel, including technical mountaineering, ski-touring, and sea-kayaking.
This history of heavy load-bearing and sustained physical demand established a high baseline of somatic resilience. Throughout his clinical history, the subject has demonstrated a remarkable capacity for neuroplastic adaptation and self-directed rehabilitation following major systemic interruptions.
History of Somatic Resilience
- Gait-Rebuilding Lifecycles: The subject has successfully navigated seven distinct lifecycles of rebuilding gait mechanics following major neurological and systemic events.
- Neuroplastic Capacity: Demonstrated ability to achieve near-complete resolution of hemiparetic symptoms through intensive, implicit motor-learning protocols.
- Systemic Recovery: Consistent history of returning to high-level physical activity (e.g., technical ascents) after acute cardiovascular and infectious crises.
2. The Deconditioning Cascade: Chronology of Systemic Interruption
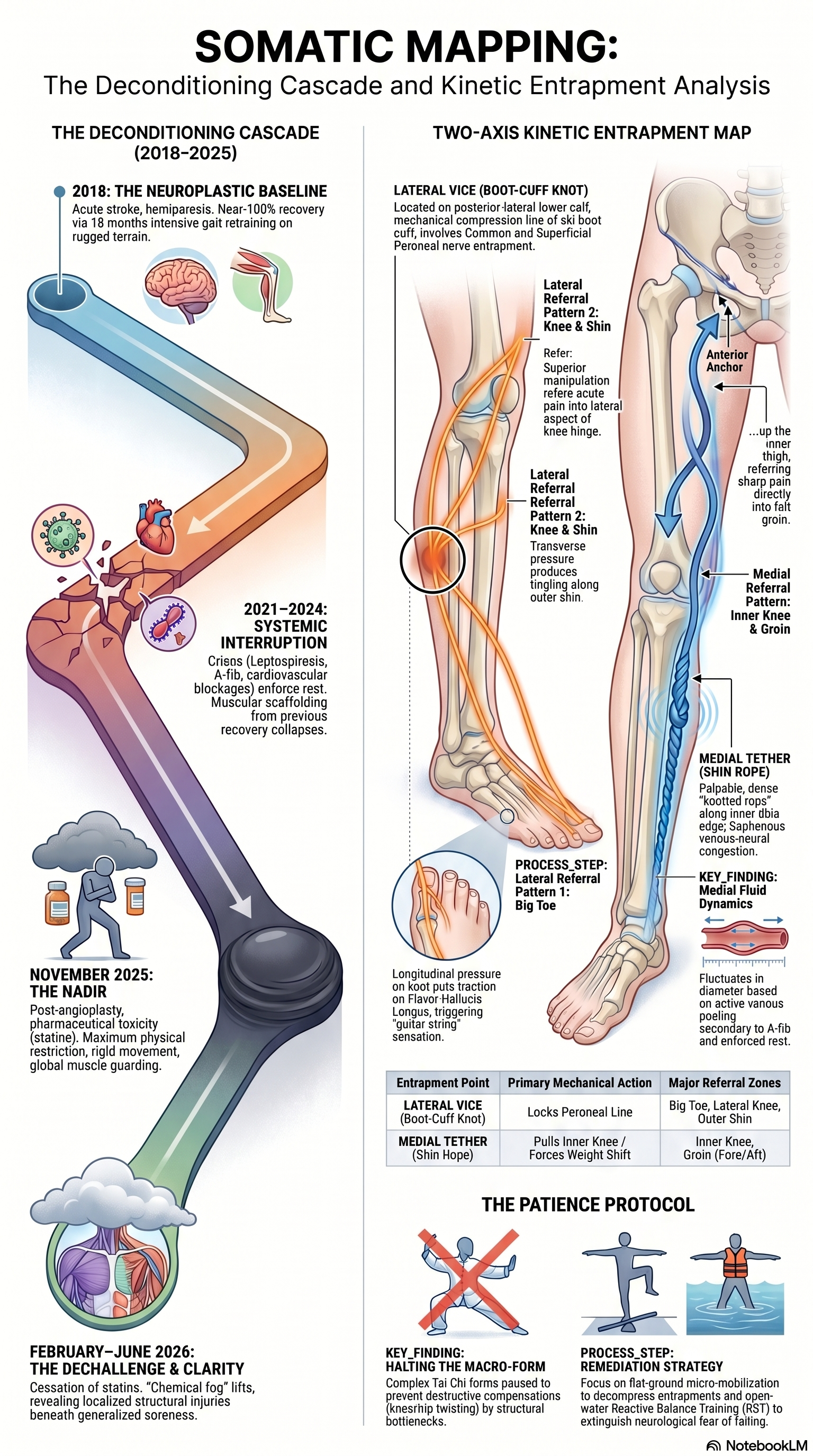
- 2018 (The Neuroplastic Baseline): Following an acute stroke, the subject presented with left-sided hemiparesis, foot-drop, and a compensatory "waddle." He engaged in an 18-month self-directed recovery protocol centred on implicit gait retraining over rugged, unpredictable terrain while walking dogs. This resulted in a 100% resolution of the foot-drop and the structural waddle, re-establishing a high-functioning baseline.
- 2021–2024 (The Interruption & Deconditioning Cascade): A cascade of systemic crises—including Leptospirosis, the onset of Atrial Fibrillation (A-fib), severe hypertension, and cardiovascular blockages—required angioplasty and stent placement. The resulting multi-year period of enforced rest caused the collapse of the muscular "scaffolding" established in 2018. This loss of stability unmasked latent mountain injuries, leading to recurrent knee-buckling and severe ankle sprains.
- November 2025 (The Nadir Baseline): Observations made four weeks post-angioplasty during a cohort parkour session—documented via video clips—captured the subject at maximum physical restriction. The subject displayed rigid, guarded movement patterns and global muscle guarding, characterized clinically as "moving like an old man," driven by surgical recovery and active pharmaceutical toxicity.
3. Pharmacological Variable: Statin-Induced Myopathy and Recovery. The clinical picture was significantly confounded by a complex pharmacological trial involving four sequential statin protocols. This exposure induced severe, toxic muscle breakdown approaching a state of clinical rhabdomyolysis.
The Dechallenge and Clearance Window
In early February 2026, a clinical "Dechallenge" was initiated, with all statin interventions ceased. A four-month "Clearance Window" was established to allow the chemical myopathy to resolve, providing a clean baseline for structural assessment.Clinical Significance of the Four-Month Mark (June 2026) By June 2026, the subject reported a dramatic lifting of the "somatic fog" and the cessation of generalized thigh soreness. This resolution was a critical diagnostic prerequisite; by clearing the global chemical noise, the "true" highly localized structural injuries—previously obscured by generalized myopathy—were finally unmasked for targeted intervention.
4. Structural Analysis: The Lateral Axis (The Boot-Cuff Knot)Assessment revealed a localized restriction point on the posterior-lateral lower calf. This entrapment occurs precisely at the mechanical compression line created by the cuff of a rigid plastic ski/mountaineering boot. The entrapment of the Superficial and Common Peroneal nerves is markedly more severe on the left (stroke-affected) limb.
Palpation Mechanics: Lateral Axis
Movement/Pressure Type | Mechanical/Neurological Output |
|---|---|
Longitudinal Pressure (Superior/Inferior) | Produces linear traction on the underlying Flexor Hallucis Longus (FHL) tendon; triggers a "guitar string" sensation terminating behind the first hallux (big toe). |
Transverse Pressure (Horizontal Friction) | Displaces deep fascial sheets (crural fascia/lateral septum); produces reciprocal tingling/burning along the Superficial Peroneal Nerve pathway (outer shin). |
Superior Tracking (Upward Manipulation) | Moving the horizontal manipulation upwards from this cuff point causes acute pain referral into the lateral knee hinge (Common Peroneal Nerve tracking around the fibular neck). |
5. Structural Analysis: The Medial Axis (The Shin Rope)The medial axis presents as a dense, palpable "knotted rope" structure running along the inner edge of the tibia, descending from the inner knee hinge. This is clinically identified as Saphenous Venous-Neural Congestion.
The Fluid Variable
The "Shin Rope" exhibits a dynamic fluid variable; its physical diameter fluctuates from the thickness of a thumb to that of a little finger. This indicates active venous pooling in the Great Saphenous Vein, secondary to the subject's history of A-fib and prolonged enforced rest.
Clinical Finding.
Digital compression of this medial "inner shin rope" transmits immediate mechanical traction through the adductor canal. This refers sharp, acute pain directly into the left groin, anchoring both fore (at the anterior ASIS) and aft (at the posterior pubic/ischial anchor).
6. Kinetic Synthesis: Reciprocal Tethering Logic. The "Two-Axis Kinetic Entrapment Map" illustrates a dysfunctional feedback loop that locks the lower leg into a state of guarded stagnation.
- The Medial Tether: The Saphenous/Shin Rope congestion pulls on the inner knee and refers pain to the groin anchors. This forces a defensive weight shift away from the medial line.
- The Lateral Vice: This weight shift increases tension on the peroneal line, where the "Boot-Cuff Knot" locks the fascia. This in turn pulls on the big toe and refers pain to the lateral knee.
- The Closed Loop: If the Medial Tether pulls, the body shifts weight; then the Lateral Vice engages, locking the peroneal line. This reciprocal relationship prevents joint fluidity and compels the subject into high-risk compensatory gait patterns.
7. Therapeutic Strategy: The "Patience Protocol"
The core thesis of the current rehabilitation phase is the deliberate cessation of macro-geometric movements. Specifically, the subject has halted execution of the Cheng Man-ch'ing 37-step short form. Clinical reasoning dictates that forcing this complex Tai Chi form while foundational bottlenecks remain will only compel the knee and hip into destructive, counterproductive compensations.Primary Intervention Modalities:
- Lower Leg Micro-mobilization: Targeted manual decompression of the medial-lateral bottlenecks to restore fascial sliding and resolve nerve entrapment.
- Reactive Balance Training (RBT): Utilization of open-water paddleboard training. This provides an unpredictable, low-impact environment to retrain neuromuscular responses and extinguish the neurological "fear of falling" without the risks associated with ground-based impact.
Clinical Outlook The subject has successfully transitioned from a state of systemic chemical myopathy to a phase of localized structural restoration. By systematically addressing the "Reciprocal Tethering" of the peroneal and saphenous lines, the protocol aims to resolve the multi-axis entrapment, restore structural fluidity, and facilitate a return to high-consequence mountain travel.
Nota Bene: These Somatic findings are by their nature ethereal. Recovery is never a linear process. The next time I carry out any deep Somatic reading & mapping, the output may change, adding yet another layer. I have spent a lifetime falling with style. Trying to encapture that into one single document is nigh on impossible.